Case Study 2 - FQHC Collaboration for Population Health - Diabetes
Private Benefit Network
Chronic Condition Intervention - Hospital
The prevalence and cost of diabetes has grown to crisis proportions in many areas of the country. By 2020, nearly half of the U.S. adult population will have either diabetes or prediabetes, with associated health care costs approaching $500 billion. Currently, over 25% of Americans above the age of 65 are diabetic. This level is estimated to double by 2050.
Aside from direct current costs of the condition (led by the cost of medications and supplies), diabetes related acute occurrences such as heart attack, stroke, vascular failure and amputation have a devastating impact on both the affected individuals, and the health plan in which they participate. In fact, total medical expenditures for individuals suffering from diabetes is double the rate of those without a diabetic diagnosis. Further, studies indicate that up to 50% of individuals with chronic health conditions are non-adherent to prescribed medication regimes. With a condition such as diabetes, failure to follow such prescribed regimes can quickly lead to catastrophic claims occurrences. Finally, through a condition which affects all economic stratums, the effects of diabetes are more heavily felt in rural and lower income populations, which often experience additional impediments to efective management, such as access to care, cultural biases and communication barriers.
In most cases the resources are in place, at least to some extent. The failure in the current system is the lack of a central collaboration function to serve as a nexus for those resources.
Enhanced education and lifestyle support are key needs in reducing both the cost and the prevalence of diabetes. Most diabetic support mechanisms in place today focus on such prevention-intensive by. These are critically important in an overall strategy, but as important as these resources are, they tend to overlook a key concern with most mature health plan arrangements, namely, clinical health management and cost control for the large blocks of current insureds suffering from uncontrolled diabetic complications.
In many instances, particularly with lower income populations, ineffective self-monitoring, lack of prescription adherence and poor access to primary care support to activate remedial strategies can result in substantially reduced health outcomes and lead to massively higher long-term claims expenses.
To meet this growing need, an integrated triage strategy is required, which identifies, engages, measures and provides care fulfillment for the most at-risk members of this demographic. The Private Benefit Network Diabetic Intervention Program (DIP) is a focused intervention strategy designed to support at-risk individuals within insured populations, combining focused condition metrics, patient home outreach and engagement, expanded condition education and enhanced RX adherence to provide better medical outcomes. DIP can either function as a standalone at-risk intervention strategy or be integrated with existing broad-based preventive care arrangements. This strategy is further enhanced by incorporating direct cost reductions on associated diabetic related pharmaceuticals and supplies, allowing self-insured health plans, MEWAs and Association Health Plans to achieve immediate cost savings, while minimizing the likelihood of catastrophic health occurrences and reducing overall long-term claims.
Diabetic Intervention Program Process
The DIP strategy uniquely spotlights the most at-risk members, with the goal of reducing or avoiding catastrophic claims events, rather than hoping for lifestyle changes. It involves four primary components.
- Directed Patient Engagement
- Focused condition management is assigned by a payer or plan to an associated Federally Qualified Heath Center (FQHC) and delivered via existing FQHC patient home infrastructure
- Following plan communications, FQHC outreaches to the patient to begin engagement process, provide condition education and coordinate delivery of glucometer and supplies
- Support is provided via Telehealth or direct delivery - optimizing patient outreach
- Metric Measurement
- Bluetooth glucometer and associated supplies are used to expedite metric capture and analysis
- Bluetooth glucometer collects data, transmits via Bluetooth to phone app, encrypts and delivers to designated FQHC
- Algorithm analyzes results against established baseline and identifies at-risk patients in real time
- Patient Home Outreach
- FQHC is provided with metric identified at-risk individuals, as well as RX adherence data
- FQHC provider, through Patient Home infrastructure, contacts at-risk individuals based on RX utilization data, monitors adherence per identified protocol and recommends follow-up action
- RX and Supply Cost
- FQHC regulatory status allows for access to diabetic RX on a reduced basis, resulting in direct, immediate RX claims cost savings to payer for meds
- Diabetic supplies associated with Bluetooth glucometer are also available at a lower net cost, resulting in a 50% reduction in cost of supplies for affected individuals
Schematic
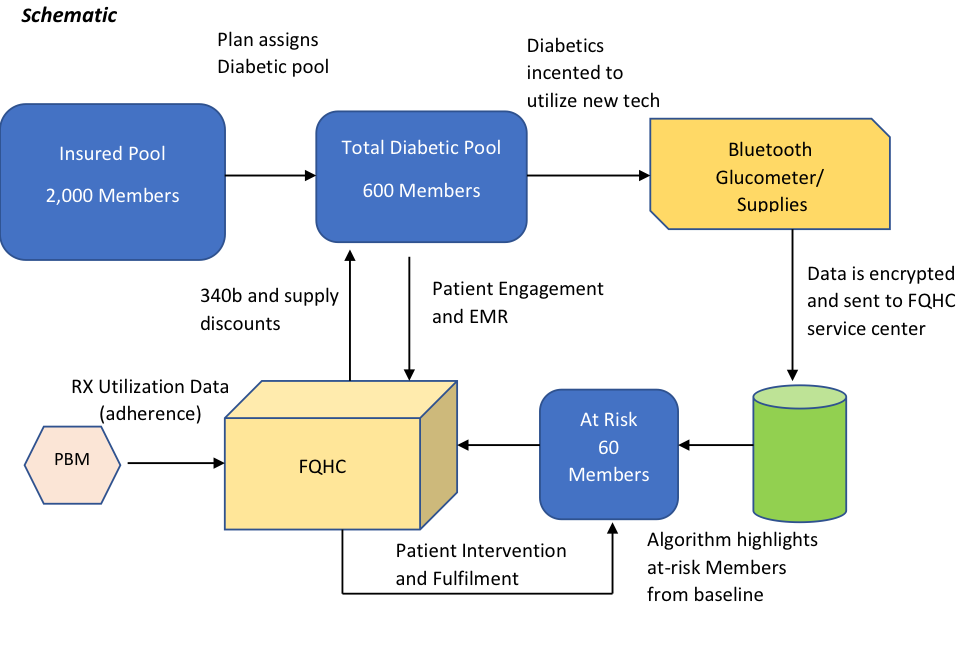
The DIP strategy utilizes existing technology and established patient outreach infrastructure to connect at-risk health populations with a provider network, which is uniquely positioned to oversee specified conditions, identify negative changes in health metrics and, when coupled with information on RX adherence, directs remedial actions to avoid long-term claims experience. Further, due to the unique regulatory nature of the FQ providers, substantial discounts are available on both required pharmaceuticals and associated supplies.
Payer/Plan Value Proposition
For payers and self-insured plans, the DIP strategy offers 2 primary avenues for substantial cost savings:
- Based on the regulatory overlay of the FQHC providers, the plan or payer has the opportunity to generate immediate savings on the cost of diabetic related pharmaceuticals for all participating members, as well as significant savings on the cost of diabetic supplies. The level of savings more than pays for any cost associated with the enhanced condition management and generates additional net current claims savings
- Based on the enhanced triage approach, medication adherence will be improved and individuals exhibiting deteriorating blood sugar indications will be identified with appropriate intervention on a current basis, rather than waiting for the next annual PC visit. This approach should result in improvements in both health outcomes and claims costs for those most at-risk in a given cohort
- Improvements in high risk metrics will directly lead to reduction in comorbidity claims, ED utilization (for non-emergent interventions), and hospital readmissions
Partner Value Proposition
Physician JV Relationships- Historically, FQHCs and local primary care physicians have had a challenging relationship. Many private practice physicians view FQHCs as direct competition for patient load, and benefiting of certain governement sponsored advantages. The DIP strategy offers the opportunity for an enhanced dynamic between primary care providers and FQHCs, capitalizing on the inherent strengths of each party, and allowing existing primary care providers (PC) to continue their existing patient relationship, while the FQHC provider takes on the expanded engagement and monitoring of disease-based metrics, sharing net results with the PC. It is also possible to structure this strategy as a value-based reimbursement arrangement, which incents both the PC and the FQHC provider for improvements in claims results, effectively creating a condition-dependent ACO-like mechanism.
Hospital JV Relationship - Similarly, the DIP program offers the opportunity for hospitals and local FQHCs to combine resources to provide enhanced population health management alternatives in their joint footprint. As with the potential physician relationships, an opportunity exists for value-based, reimbursement payments based on improved metrics to both the hospital and the FQHC provider.
Public Health - Significant existing resources have been expended by Public Health Agencies to attempt to reduce the impact of diabetic conditions for given populations. Though highly valuable, many of these services fail to generate optimal results. This is often not due to a lack of resources, but rather to a lack of effective coordination and triage capabilities. The DIP program represents an opportunity to enhance results of existing initiatives with broader community coordination and meaningful provider intervention.
Medicare Advantage Opportunities - Given the high incidence of diabetes in the post 65 population, the DIP strategy creates an excellent avenue for reducing net cost differentials for existing and new Medicare Advantage arrangements, creating additional claims savings vs. established CMS reimbursement guidelines
Back to Case Studies



